
Research Review: Low Back Pain and Its Relation to the Hip and Foot
By Amy Martinez DPT, PT
Edited by Brent Brookbush DPT, PT, COMT, MS, PES, CES, CSCS, ACSM H/FS
Original Citation: Cibulka, M. T. (1999). Low back pain and its relation to the hip and foot. Journal of Orthopaedic & Sports Physical Therapy, 29(10), 595-601. - ARTICLE
Introduction: Research has demonstrated a correlation between a loss of hip rotation range of motion (ROM) and low back pain (1-3). An asymmetrical loss of hip external ROM has been correlated with sacroiliac joint dysfunction (SIJD) (4-7). SIJD has been shown to increase the likelihood of other asymmetries, such as subtalar joint pronation (8-9). This 1999 case study by an American researcher demonstrates a relationship between SIJD , asymmetrical hip rotation ROM and subtalar joint pronation in an individual with unilateral LBP. This study may suggest that ankle, hip and SIJ dysfunction should be assessed and addressed in those with low back pain.

Resisted Walking - Example of a lower extremity "Integration Exercise"
Study Summary
| Study Design | Case study |
| Level of Evidence | III Evidence from non-experimental descriptive studies, such as comparative studies, correlation studies and case-control studies |
| Participant Characteristics | Demographics
Inclusion Criteria:
Exclusion Criteria:
|
| Methodology |
|
| Data Collection and Analysis |
|
| Outcome Measures |
|
| Results |
|
| Our Conclusions | This case study describes relationships similar to those described in Lumbo Pelvic Hip Complex Dysfunction (LPHCD), Sacroiliac Joint Dysfunction (SIJD) and Lower Extermity Dysfunction (LED). Further, the participant's unilateral pronation demonstrates the importance of a dynamic postural assessment, such as the overhead squat assessment, to determine the full extent of asymmetries and compensation patterns in those exhibiting signs of LBP and/or SIJD. |
| Researchers' Conclusions | In this case study, the participant exhibited low back pain and asymmetry in hip rotation ROM. Sacroiliac joint dysfunction with unilateral excessive hip lateral rotation and unilateral excessive subtalar joint pronation were demonstrated on the same side. These findings suggest a correlation between low back symptoms, hip and lower extremity dysfunction. |
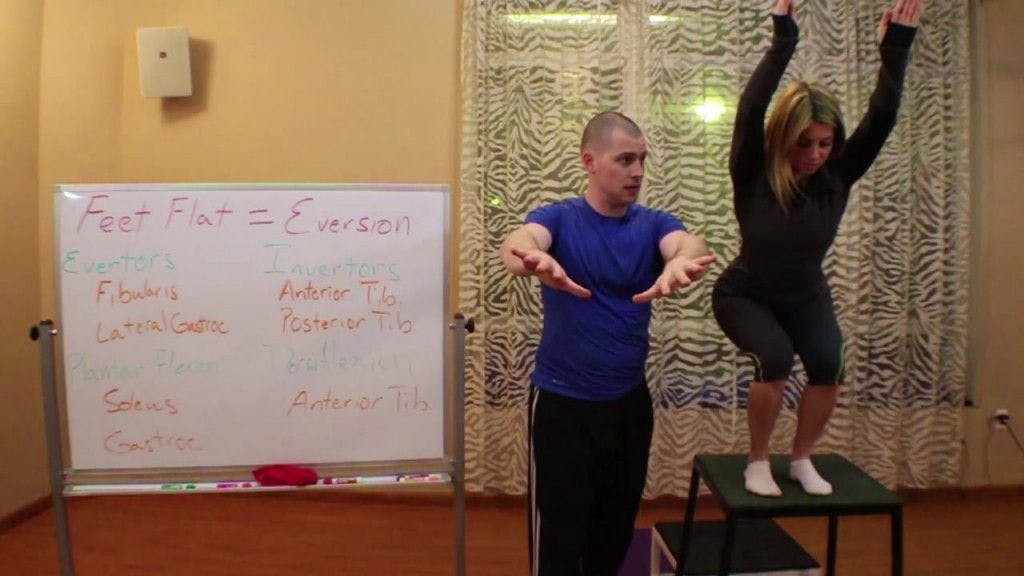
Overhead Squat Assessment - demonstrating feet flattening (pronation). (Image: Courtesy of www.BrentBrookbush.com)
How this study contributes to the body of research:
This case study on an individual with unilateral low back pain (LBP) examined hip rotation range of motion (ROM), signs of sacroiliac joint dysfunction (SIJD ) and subtalar joint position. Previous studies demonstrated correlation between low back pain (LBP) and SIJD , SIJD and asymmetry in hip external rotation ROM (4-7), SIJD and subtalar joint pronation (8-9), or LBP and excessive hip lateral rotation (8,10). Unique to this study, the researcher demonstrated that an individual with unilateral low back pain may exhibit all of these impairments. These findings may imply a correlations between LBP, SIJD , asymmetry in hip rotation ROM (specifically excessive hip external rotation) and subtalar pronation, or perhaps a compensation pattern that includes these signs and additional maladaptive changes in motion.
How the Findings Apply to Practice:
The findings of this case study imply that there may be an association between sacroiliac joint dysfunction (SIJD ), asymmetry in hip external rotation range of motion (ROM) and unilateral subtalar pronation. This suggests that individuals with unilateral low back pain (LBP) should be assessed for SIJD , asymmetries in hip ROM, and subtalar position/motion. Further, human movement professionals should be prepared (have a repertoire of techniques) to address any dysfunction noted at these three joints, despite the hip and subtalar joints being distal from the area of patient complaint.
The study had many methodological strengths, including:
- The researcher used the Oswestry low back pain disability questionnaire as a functional outcome measure, enhancing the validity of the results.
- The participant was observed for one year, providing both short-term and long-term results of the intervention plan.
- The SIJD special test methods were common special tests and were clearly described; enhancing replicability of the study and clinical applicability.
Weaknesses that should be noted prior to clinical integration of the findings include:
- A ‘gold standard’ for detecting movement dysfunction of the sacroiliac joint does not exist. SIJD movement assessment are heavily reliant on palpation, which may reduce reliability.
- The researcher visually assessed trunk range of motion; an objective, reliable continuous interval measure (example, bubble goniometry) may have increased reliability.
- This study was a single-subject case study; this is a weaker form of evidence that is likely best considered a potential finding that should be verified by larger studies.
How the study relates to Brookbush Institute Content
The Brookbush Institute (BI) has developed predictive models of postural dysfunction based on evidence of common tissue changes (muscle, joint, fascia and nerve) to aid human movement professionals in selecting optimal assessments, manual interventions and exercise. This case study describes relationships similar to those described in Lumbo Pelvic Hip Complex Dysfunction (LPHCD) , Sacroiliac Joint Dysfunction (SIJD) and Lower Extermity Dysfunction (LED) . Further, this study demonstrates the importance of a whole body dynamic postural assessment, such as the overhead squat assessment , to determine the full extent of asymmetries and compensation patterns in those exhibiting signs of LBP and/or SIJD.
The following videos illustrate common assessment techniques for the LPHCD and SIJD :
Overhead Squat Assessment: Sign Clusters – Lumbo Pelvic Hip Complex Dysfunction
Overhead Squat Assessment: Sign Clusters – Feet Flat Breakdown
Goniometry: Hip external rotation in prone
Goniometry: Hip internal rotaiton in prone
Stork Test: Special Test for SIJ Motion
Bibliography:
- Barbee Ellison, J., Rose, S. J., & Sahrmann, S. A. (1990). Patterns of hip rotation range of motion: a comparison between healthy subjects and patients with low back pain. Physical Therapy, 70(9), 537-541.
- Mellin, G. (1988). Correlations of hip mobility with degree of back pain and lumbar spinal mobility in chronic low-back pain patients. Spine, 13(6), 668-670.
- Chesworth, B. M., Padfield, B. J., Helewa, A., et al. (1994). A comparison of hip mobility in patients with low back pain and matched healthy subjects. Physiother Can, 46, 267-274.
- LaBan, M. M., Meerschaert, J. R., Taylor, R. S., & Tabor, H. D. (1978). Symphyseal and sacroiliac joint pain associated with pubic symphysis instability. Archives of physical medicine and rehabilitation, 59(10), 470-472.
- Cibulka, M. T. (1992). The treatment of the sacroiliac joint component to low back pain: a case report. Physical therapy, 72(12), 917-922.
- Fowler, C. (1986). Muscle energy techniques for pelvic dysfunction. Modern Manual Therapy of the Vertebral Column. Edinburgh, Scotland: Churchill Livingstone, 805-14.
- Cibulka, M. T., Sinacore, D. R., Cromer, G. S., & Delitto, A. (1998). Unilateral hip rotation range of motion asymmetry in patients with sacroiliac joint regional pain. Spine, 23(9), 1009-1015.
- Botte, R. R. (1981). An interpretation of the pronation syndrome and foot types of patients with low back pain. Journal of the American Podiatry Association, 71(5), 243-253.
- Rothbart, B. A., & Estabrook, L. (1988). Excessive pronation: a major biomechanical determinant in the development of chondromalacia and pelvic lists. J Manipulative Physiol Ther, 11(5), 373-9.
- Gross, M. T. (1995). Lower quarter screening for skeletal malalignment—suggestions for orthotics and shoewear. Journal of Orthopaedic & Sports Physical Therapy, 21(6), 389-405.
© 2018 Brent Brookbush
Questions, comments, and criticisms are welcomed and encouraged.