Original Citation: Hess, S., Richardson, C., Darnell R., Friis P., Lisle D., Myers P. (2005) Timing of Rotator Cuff Activation During Shoulder External Rotation in Throwers With and Without Symptoms of Pain. J Orthop Sports Phys Ther. 35:812-820. Article
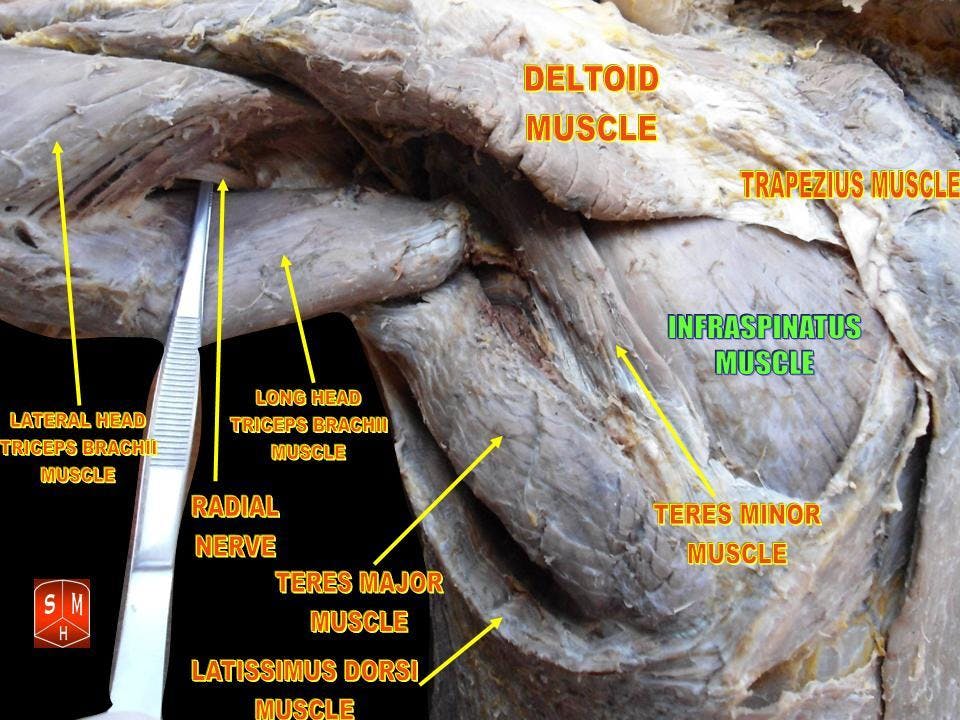
Caption: Cadaver dissection depicting a posterior view of the musculature of the shoulder with labels (infraspinatus, teres minor, teres major, trapezius, etc.)
By Anatomist90 - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=17900187
Why is this relevant?: The architecture of the shoulder joint is better suited for mobility than stability. Further, the joint capsule does not enhance stability significantly as it is relatively thin and slack in resting position. Joint stability is primarily accomplished via musculature, of particular importance to joint stability are the rotator cuff muscles (supraspinatus , subscapularis , infraspinatus and teres minor ). Previous studies have shown pain alters shoulder muscle recruitment patterns (1-2). This study investigated rotator cuff recruitment patterns in overhead athletes with and without shoulder pain, with the intent of aiding in the design of prehabilitation and rehabilitation programs.
Study Summary
Study Design
Case-Control Study with Matched Subjects
Level of Evidence
III: Evidence from non-experimental descriptive studies, such as comparative studies, correlation studies, and case-control studies
Subject Demographics
Age and Gender, and Participant Characteristics:
Asymptomatic (CON)
Total - 11 males
Mean age (Range in years) - 32.5 (24-41)
Mean height (in cm) - 178.5 (170-186)
Mean mass (in kg) - 79.9 (62-110)
Shoulder Pain (SP)
Total - 12 males
Mean age - 29.5 (22-41)
Mean height - 180 (170-195)
Mean mass - 83.8 (75-93)
Methods and Experimental Protocol:
Prior to Onset of Study
Each participant filled out a Habitual Activity Questionnaire.
A Modified Rowe Score was calculated for each participant to estimate level of functional disability
CON - excellent status
SP - Fair-to-good status
Physical examination of each participant was done by a Physical Therapist (PT) and sports physician (MD)
Tests included range of motion (ROM) of the shoulder, shoulder instability and impingement assessments (Anterior and Posterior Drawer Tests; Apprehension and Relocation Tests; Hawkins-Kennedy
Impingement Test)
Visual Analog Scale (VAS) pain levels were collected prior to testing for each participant
Data Collection Protocol
Fine-wire bipolar electrodes were inserted (with ultrasound guidance) into the muscle bellies of each of the rotator cuff muscles of the participant's throwing arm (supraspinatus, infraspinatus, and subscapularis)
In order to measure movement speed in the sagittal plane, an accelerometer was placed on the forearm.
Premotor reaction time test (RTT) was performed for each participant
Participant was positioned in sitting with the arm supported at 90° of shoulder abduction and 90° of elbow flexion with the palm resting on the plinth
The participant was passively moved through the desired testing motion (90° of shoulder external rotation and 90° of shoulder abduction with 90° of elbow flexion) by the researchers
Speed of completion for the movement was emphasized verbally by the researchers
Initiation of movement began after the light flashed
3 trials of shoulder external rotation were performed prior to testing for familiarization with the movement
10 repetitions of shoulder external rotation were performed in tandem with the flickering light, which was randomly set to flash at different time intervals
Inclusion Criteria:
Competitive baseball players who played at least once per week and trained at least twice per week
Report symptoms of shoulder pain during throwing activities in training and game situations
Exclusion Criteria:
General Exclusion Criteria
Any cervical, thoracic, or upper limb injury or problems that required surgery
Any previous fracture of the cervical or thoracic spine, shoulder and upper limb
Any previous shoulder dislocations
Any neurological or respiratory conditions
For SP Group
Any signs or symptoms of cervical, thoracic, or upper limb pain other than specific shoulder pain
Pain levels of > 1 during testing by visual analog scale
For CON Group
Any cervical, thoracic, shoulder, or upper limb pain during the past year
Any previous cervical, thoracic, or upper limb injury in the past that required any medical intervention
Outcome Measures
Primary Outcome Measures
Timing of the onset of EMG activity in relation to the light flash
Relative latency of the onset of EMG activity in relation to the agonist muscle (infraspinatus in this study, as external rotation was performed)
Secondary Outcome Measures
Comparison of physical exam findings between groups (this data was not analyzed, just observed and correlated with primary outcome measures)
Subscapularis was the first muscle to fire in the CON group, occurring 50 milliseconds prior to the onset of the movement into external rotation whereas in the SP group subscapularis tended to be the last muscle to fire after infraspinatus and supraspinatus .
Physical examination findings in the SP group suggested increased prevalence of instability of the shoulder girdle complex.
Conclusions of the Researchers
The presence of shoulder pain significantly alters motor recruitment patterns of the rotator cuff, disrupting glenohumeral joint stability.
Caption: Dr. Brookbush teaches a client how to perform rotator cuff reactive activation using a bodyblade, with cuing to reciprocally inhibit the supraspinatus and posterior deltoid.
Rotator Cuff Reactive Activation/Integration
Review & Commentary:
The current study exhibits strengths in its methodology. First, each of the group's participants was appropriately paired at baseline. Pairing between groups allows researchers to compare the effect of one variable (shoulder pain) on muscle firing patterns in otherwise similar individuals, isolating shoulder pain's effect on rotator cuff activity. Second, the data collection procedure was described clearly and succinctly which aids in replication of the study in the future (more on this below). Of note, the clinical shoulder examination allows the researchers to link results (delayed EMG firing of subscapularis in participants with shoulder pain) in the external rotation task to clinical presentation (anterior instability) of the participants, strengthening the researchers' conclusion. Last, intramuscular electrodes are more specific than surface EMG electrodes. Intramuscular electrodes are useful for examining rotator cuff muscle activity due to the location and depth of the muscles while reducing the chance of picking up adjacent muscle activity (such as from trapezius , rhomboids , posterior deltoid , and/or latissimus dorsi ).
The current study also had weaknesses in its methodology. Although intramuscular fine-wire needling is specific, it only records local motor units. Previous research has shown muscles can be regionally activated, including the subscapularis (3-4). Future studies should investigate different fiber bundles of the subscapularis to determine if the pattern of activity observed can be generalized to the entire muscle. Second, no EMG analysis of the magnitude of the rotator cuff muscle activity was reported. Scovazzo et al. previously reported changes in the amount of muscle activity and firing pattern of swimmers with shoulder pain (2). Future studies may attempt to correlate the relative amount of activity and timing of muscle recruitment in those with shoulder pain across various sports.
Why is this study important?
The current study adds to the body of literature, indicating the presence of pain alters muscle activity and firing patterns. Specifically, this study indicates the presence of shoulder pain compromises the dynamic stabilization of the humerus in an external rotation task, by altering the timing of rotator cuff muscle recruitment. In normal participants, the subscapularis fires before the other rotator cuff musculature to help prevent excessive anterior humeral head migration. In participants with shoulder pain, the subscapularis fires after other rotator cuff muscles, decreasing the stability of the shoulder joint .
How does it affect practice?
The glenohumeral joint relies on the synchronized activation of the rotator cuff muscles to stabilize the humeral head during motion. Results of the current study show delayed activation of the subscapularis in an external rotation task in individuals with shoulder pain. With respect to the results of the current study, subscapularis isolated activation could be indicated in overhead athletes with shoulder pain. Although not reported in the results, visual observation of the graph depicting EMG activity of each of the rotator cuff muscles seemed to suggest delayed and increased firing of subscapularis in individuals with shoulder pain, indicating some degree of over-activity. Future studies are needed to confirm the magnitude of subscapularis activity. Changes (increase or decrease in activity) in magnitude, may influence intervention selection; for example, over-active with latent firing may imply release and reactive activation exercises.
How does it relate to Brookbush Institute Content?
Typically, in Upper Body Dysfunction (UBD) the subscapularis is classified as "short/overactive," requiring release and lengthening techniques. However, the results of the current study suggest that in overhead athletes with shoulder pain, the subscapularis may be classified as "long/underactive." Diagnostic testing resulted in positive signs for anterior instability in all of the individuals assigned to the "shoulder pain" group. It is likely, and has been previously noted by the Brookbush Institute, that "Anterior Instability" may be a variation of UBD , requiring a separate model and modification to the recommended interventions (similar to "Functional Varus" relative to Lower Leg Dysfunction (LLD)) . In all cases of UBD , stability of the glenohumeral joint via neuromuscular re-education of the rotator cuff is a priority. The Brookbush Institute recommends interventions based on movement assessment, including the Overhead Squat Assessment , goniometry , manual muscle testing , and passive accessory motion exam. Appropriately synthesizing clinical findings from these assessments will lead to optimal intervention and exercise selection. Future studies are needed to further clarify the pattern of subscapularis activity in overhead athletes with shoulder pain, and how that activity changes following various interventions. The following videos are an introduction to the assessments and common interventions used by the Brookbush Institute for shoulder dysfunction.