Original Citation: Park HB, Yokota A, Gill HS, El Rassi G et al. (2005). Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am. 87(7): 1446-1455. ABSTRACT
Why is this relevant?: Rotator cuff tears, glenohumeral joint instabilities, and labral tears are associated with an increased incidence of subacromial impingement (1). The "cluster" of tests validated to rule in/rule out subacromial impingement only indicates the presence or absence of impingement (1). There is a need for a definitive cluster of tests to identify pathologies that may present with subacromial impingement. The current study investigated 8 different clinical tests to determine an optimal testing cluster to differentiate individuals with varying degrees of subacromial impingement secondary to rotator cuff pathology (rotator cuff tear with impingement).
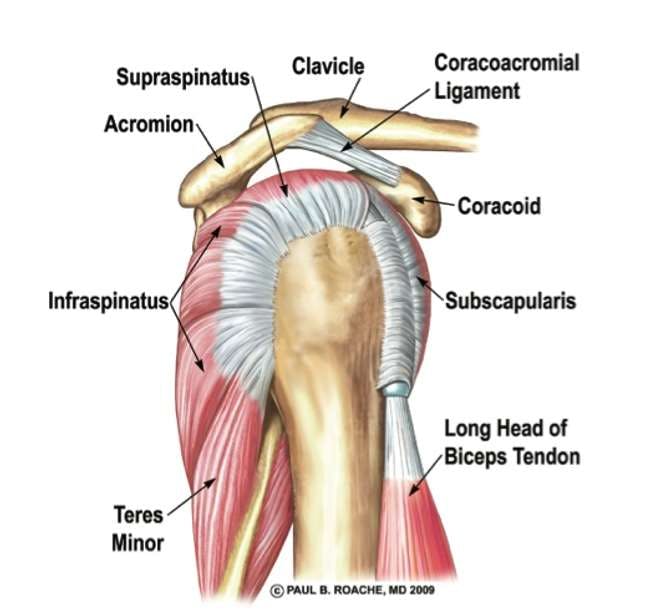
Caption: Illustration of the lateral view of the glenohumeral joint with the infraspinatus, teres minor, subscapularis, supraspinatus labeled.
The rotator cuff has an important role in providing glenohumeral joint stability. The presence of a rotator cuff tear can predispose an individual to subacromial impingement and shoulder pain.
Study Summary
Study Design
Case Control Prospective Design
Level of Evidence
III Evidence from non-experimental descriptive studies, such as comparative studies, correlation studies, and case-control studies
Subject Demographics
Between 1992-June 2003, 1,127 patients who were scheduled for arthroscopic shoulder surgery provided a history, filled out a questionnaire, and underwent a complete physical examination within 4 weeks of surgery. Each patient had radiographic images taken of the shoulder from various angles. 214 of the 1,127 patients were excluded from further analysis because they did not undergo surgery. An additional 361 were excluded for various reasons including a previous history of shoulder surgery (n = 126), distal clavicle resectioning with a rotator cuff repair (n = 73), incomplete physical examination secondary to pain or lack of range of motion (n = 63), labral tears (n = 57) and glenohumeral joint instabilities (n = 42). In total, 552 patients were included in the final analysis.
Age: not specified
Gender: not specified
Characteristics (Protocol):
Description of the impingement tests used:
Neer's test: The examiner stabilized the scapula with the involved shoulder flexed to full elevation or reports of pain. Pain in the anterior or lateral part of the shoulder in the range of 90°-140° was considered a positive test.
Hawkin's-Kennedy test: The involved shoulder was placed in 90° of elbow and shoulder flexion and maximally internally rotated. Pain during internal rotation was considered a positive test.
Painful arc test: The examiner asked the patient to actively elevate the involved shoulder in the scapular plane until full elevation was reached. The patient was then instructed to lower the arm down. Pain or painful catching between 60°-120° of shoulder elevation was considered a positive test.
Supraspinatus muscle strength test (empty can test): The patient elevated the affected shoulder to 90° and the examiner positioned the arm into internal or neutral rotation. The examiner resisted abduction of the affected arm. The test was considered positive if the patient's arm gave way to the resistance.
Speed test: The elbow of the affected arm was maximally extended and the arm was elevated (actively or passively) and extended horizontally. With the forearm supinated, the examiner applied a downward force to the arm. Pain during forward elevation was considered a positive test.
Cross-body adduction test: The affected arm was placed in 90° of forward flexion and was passively adducted across the body by the examiner. Pain in the shoulder during passive adduction was considered a positive test.
Drop-arm test: The patient elevated the affected arm fully and then was asked to slowly lower it down under control. Severe pain or uncontrolled lowering of the arm was considered a positive test.
Infraspinatus muscle strength test: The patient's elbow was flexed to 90° and the arm was adducted to the trunk in neutral rotation. The examiner applied an internal rotation force to the distal forearm while the patient resisted. Pain, severe weakness, or an external rotation lag sign were considered positive test results. External rotation lag sign was observed when the patient could not maintain external rotation with the shoulder and elbow flexed to 90°. A positive test was the shoulder moving into internal rotation.
After arthroscopic examination to determine presence or absence of subacromial impingement, the 552 patients were divided into a non-impingement group (n = 193) and an impingement group (n = 359).
Non-impingement group had normal rotator cuffs (RTC) but presented with concomitant shoulder pathology including instability (n = 158), isolated degenerative acromioclavicular arthritis (n = 26), supraspinatus ganglion cyst (n = 5), nonspecific synovitis (n = 3), superior labral anterior-to-posterior lesion (n = 1).
Impingement group consisted of patients diagnosed with impingement, regardless of the severity of the RTC lesion. All patients in this group had a history of pain in the deltoid region or pain radiating down the arm that resolved (temporarily) with a subacromial injection of local anesthetic. These patients were sub-divided again according to the degree of RTC muscle degeneration/tears.
Group 1 (n = 72) - consisted of patients who had positive impingement tests but no RTC disease at the time of surgery.
Group 2 (n = 72) - Consisted of patients who were diagnosed with a partial RTC tear at the time of surgery, regardless of the depth of the tear. This group included bursal tears (5), and joint-sided partial tears (67).
Group 3 (n = 215) - Consisted of patients with a full-thickness RTC tear, regardless of the size of the tear.
Statistical Analyses Performed
Sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy of the 8 tests were calculated.
A forward stepwise logistic regression analysis was performed to determine the best combination of clinical test for predicting the various grades of impingement syndrome. Level of significance was set at p ≤ 0.05.
Inclusion Criteria: See above
Exclusion Criteria: See above
Outcome Measures
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy (compared with arthroscopy) of the 8 different tests performed
Determining the best combination of clinical tests for predicting the various grades of impingement syndrome.
Results
Overall Diagnostic Values of the Eight Clinical Tests for Subacromial Impingement Syndrome Regardless of the Severity of Rotator Cuff Disease
Group 3 - Painful arc test was the most sensitive test (75.8%) and had the highest negative predictive value (76.4%) whereas the drop-arm test was most specific (87.5%). The infraspinatus muscle strength test and the supraspinatus muscle strength test had the highest positive predictive values (69.1% and 68.0%, respectively) with the highest overall accuracy (~70% each). The painful arc test , the drop-arm test , and infraspinatus muscle strength test had the best post-test probability (91%) and also had a very low post-test probability if all three tests were negative (9%).
Conclusions
The best combination of tests to detect subacromial impingement of any degree are a positive Hawkins-Kennedy test , a painful arc test , and infraspinatus muscle strength tests . Post-test probabilities indicate that an individual who tests positive for all three will have a 95% chance of having some degree of RTC tear and subacromial impingement. Conversely, if these three tests were negative, that individual would have less than 24% chance to have impingement syndrome of any severity.
Conclusions of the ResearchersThe severity of RTC pathology will change the diagnostic utility of the clinical tests used to detect subacromial impingement. Clinicians should account for the variability of these tests when evaluating individuals suspected of RTC involvement.
Caption: The painful arc test can help determine the integrity of the rotator cuff musculature, specifically supraspinatus. A positive test is the inability of the individual to lower their arm under control from 90 degrees of shoulder abduction.
The drop arm test can help determine the integrity of the rotator cuff musculature, specifically supraspinatus. A positive test is the inability of the individual to lower their arm to their side under control from 90 degrees of shoulder abduction.
Review & Commentary:
This study investigated the diagnostic utility of 8 commonly used subacromial impingement tests in individuals with varying degrees of rotator cuff (RTC) pathology. The purpose of the study was to validate a cluster of tests that could be used to distinguish degrees of RTC tears in individuals with subacromial impingement syndrome.
The current study had strengths to its methodology. This study is one of the first to look at the diagnostic utility of commonly used subacromial impingement tests in three distinct groups of people: those with no RTC tears, those with small/partial RTC tears, and those with full thickness RTC tears. Implications to clinical practice are discussed below. The prospective design of the study (over an 11 year time-frame) allowed a single examiner to perform all assessments used for analysis, reducing inter-rater discrepancies. The examiner was also blinded to the patient's shoulder pathology at the time of the assessment which minimizes observer bias. Last, the large sample size of 552 patients provides adequate statistical power to make determinations about the efficacy of the clusters.
There were limitations to the study that should be mentioned prior to integration into clinical practice. Force application measurements for strength assessments such as the infraspinatus muscle strength test were not standardized across patients. The absence of force standardization is important to consider as it could alter clinical decision-making (judging a test as "positive" versus "negative") and reduce chances of an appropriate diagnosis. Similarly, the judgment of the arm "giving way" in the supraspinatus muscle strength test should have been qualified/quantified in the methodology. There were several commonly used tests that were not included in this study, such as the lift-off test (used to test subscapularis muscle integrity). The inclusion of other RTC tests could potentially lead to increased sensitivity or specificity of an RTC tear diagnostic cluster, and should be considered in future research. Last, clinicians should be careful in extrapolating the results of the current study to other patient populations, as most patients in this sample had complete RTC tears. This is not indicative of the actual prevalence of full RTC tears, and the reliability, specificity and sensitivity of these tests (clusters) may vary greatly for other populations. For example, patient populations that include overhead athletes or individuals with painful multi-directional instability may result in far more false positives. Future studies should investigate the diagnostic utility of these tests in other patient populations. Despite these limitations, the study's findings has important clinical implications and utility in the detection of RTC pathology in individuals with subacromial impingement.
Why is this study important?
Subacromial impingement may be secondary to partial or full thickness rotator cuff (RTC) tears. As rotator cuff pathology may result in precautions, the exclusion of specific interventions, or implicate the need for further diagnostic testing/medical intervention, it is important that the human movement professional has a means of differentiating primary subacromial impingement syndrome from subacromial impingement syndrome secondary to RTC pathology. The current study reports on the diagnostic utility of clusters of tests that can be used to differentiate degrees of RTC pathology present with subacromial impingement.
How does it affect practice?
The best combination of tests to detect subacromial impingement with RTC tear of any degree are the Hawkins-Kennedy test , painful arc test , and infraspinatus muscle strength tests . Individuals who test positive for all three tests have a 95% chance of having subacromial impingement; whereas, all three tests being negative results in less than a 24% chance of having impingement syndrome of any severity.
Further research is needed to differentiate partial RTC tears from full-thickness tears.
How does it relate to Brookbush Institute Content?
It is hypothesized that subacromial impingement syndrome (SIS) is the result of arthrokinematic dyskinesis of the glenohumeral joint , resulting in irritation/inflammation of subacromial tissues and pain. Further, this arthrokinematic dyskinesis is likely the result of one or more of a predictable set of compensations described in the Brookbush Institute predictive model of Upper Body Dysfunction (UBD) . As this impairment involves multiple joints, muscles, nerves and fascial structures, a thorough movement assessment is recommended before recommending an intervention/corrective program. Testing clusters, like the one discussed in this study, are used by the Brookbush Institute to “clear” the patient/client for further assessment and treatment/exercise with a licensed practitioner. Although the results of the testing cluster may not imply specific interventions, they decrease the likelihood that a patient/client’s time, financial resources, motivation and health are squandered on a conservative intervention that cannot be effective based on the nature of the pathology. In the case of the Park et al. SIS/RTC Testing Cluster , ruling out RTC pathologies by testing negative on 3 or more tests combined with an unremarkable subjective assessment, would imply that a patient/client is likely to improve under our care (Physical Therapists, Athletic Trainer, Chiropractor).
The videos below describe, demonstrate and discuss the tests used in this study:
Brookbush Institute Videos
Park et al. Rotator Cuff Tear with Subacromial Impingement Testing Cluster
Hawkins Kennedy
Painful Arc Test
External Rotation Resisted Strength Test (Infraspinatus Muscle Weakness Test)