Original Citation: Michener LA, Walsworth MK, Doukas WC, Murphy KP. (2009). Reliability and diagnostic accuracy of 5 physical examination tests and combination of tests for subacromial impingement. Arch Phys Med Rehabil. 90: 1898-1903. ABSTRACT
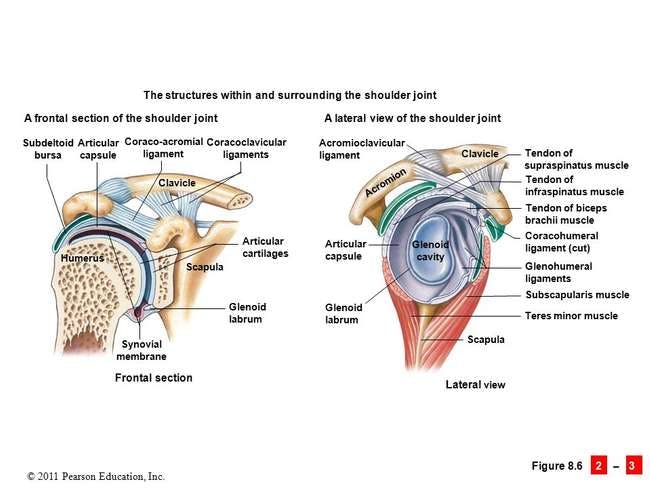
Caption: Color illustration of Internal Shoulder with non-contractile tissues labeled.
The Shoulder - Notice the numerous stuctures between the acromion and coracoacromial ligament and the humerus (subacromial space).
Why is this relevant?: Subacromial impingement syndrome (SIS) is a common shoulder conditions producing pain, weakness, and a loss of range of motion. Shoulder pain has been linked to altered muscle firing patterns and altered scapular kinematics (1-5). A diagnosis of SIS generally indicates pain is produced when subacromial structures are compressed by approximation of the humeral head (potentially the greater tubercle) and the underside of the acromion and coracohumeral ligament. Many tests have been developed to assist in the diagnosis of SIS, but more recent research has suggested many of these tests have poor sensitivity and specificity, decreasing the likelihood of an accurate diagnosis. To increase the likelihood of an accurate diagnosis, "clustering" tests has been suggested. The current study investigated 5 commonly used SIS tests to determine if a particular cluster of tests would have adequate sensitivity and specificity to positively detect SIS for individuals with shoulder pain.
Study Summary
Study Design
A prospective, single-blinded study design
Level of Evidence
III Evidence from non-experimental descriptive studies, such as comparative studies, correlation studies, and case-control studies
Subject Demographics
Age and Gender and Additional Characteristics of the Participants:
Each participant underwent a standardized history and physical examination by two different clinicians. Both clinicians were blinded to the results of the other's physical examination.
One clinician was a board certified orthopedic surgeon with 17 years of experience in management of musculoskeletal conditions
One clinician was a physical therapist board certified in orthopedics with 8 years of experience in management of musculoskeletal conditions
Each physical examination included 5 of the following tests
After both examinations were completed, each participant underwent arthroscopic examination by an independent investigator blinded to the examination results of the principal investigators.
Data analysis
Kappa coefficients and percent agreement were calculated for each test to determine inter-tester reliability between the two clinicians.
Arthroscopic findings were compared to physical examination results of the clinicians to determine the diagnostic accuracy of each of the physical examination tests.
A binary regression analysis was used to determine the tests, or clusters of tests used, that could predict the presence or absence of SIS. A ROC curve analysis was done to determine the threshold of a number of positive tests that discriminated between individuals with and without SIS.
An a priori power analysis was performed to determine the sample size needed to show statistical significance based on an effect size of 0.25 (small effect size) and power of 0.80. 57 participants were needed.
Inclusion Criteria:
Shoulder pain for more than one week
Shoulder pain was primary complaint
Exclusion Criteria: N/A
Outcome Measures
Prevalence of SIS in the participant population
Inter-tester reliability of the physical examination tests
Cluster of tests to rule in/rule out SIS
Results
Prevalence of SIS in the study:
16/55, or 29% tested positive for SIS
Only 1 had SIS alone with no other shoulder pathologies
The most common shoulder pathologies observed in the (+) SIS group were labral tears (11/16), partial rotator cuff tears (4/16), and full rotator cuff tears, biceps tendon tears, or acromioclavicular degenerative joint diseases (3/16 for each)
The most common shoulder pathologies observed in the (-) SIS group were glenohumeral joint instabilities, glenoid labral tears, and rotator cuff tears.
Inter-tester reliability of the physical examination assessments:
Hawkins-Kennedy test - Kappa coefficient and 95% CI - 0.39 (0.12-0.65), 69% agreement between clinicians
Neer's test - 0.40 (0.13-0.67), 71% agreement between clinicians
Painful arc test - 0.45 (0.18-0.72), 73% agreement between clinicians
Empty can test - 0.47 (0.22-0.72), 76% agreement between clinicians
ERRT - 0.67 (0.40-0.94), 87% agreement between clinicians
Diagnostic Accuracy For Impingement Shoulder Tests:
Less than three positive tests (out of the five investigated) are needed to rule out SIS. Specifically, the cluster identified to have the greatest ability to rule out SIS were a negative Neer's test, ERRT, and painful arc test.
Conclusions of the Researchers
The presence of a painful arc and positive ERRT and empty can tests provide diagnostic support for the presence of SIS.
Clustering the physical exam findings with the subjective history of the patient likely provides the highest sensitivity and specificity for detecting SIS.
Caption: The empty can test is one of the tests used in the Michener et al. study to identify subacromial impingement syndrome along with external rotation resistance weakness, and the presence of a painful arc.
The empty can test is one of the tests used in the Michener et al. study to identify subacromial impingement syndrome along with external rotation resistance weakness, and the presence of a painful arc.
Review & Commentary:
The primary objectives of the current study were:
Determining the inter-rater reliability of common tests used to detect subacromial impingement syndrome (SIS)
Determine the diagnostic accuracy of the individual tests
Determine an optimal cluster of tests to confirm or rule-out SIS
This study was one of the first in orthopedic and physical therapy literature to validate SIS physical exam findings with arthroscopic assessments in individuals with shoulder pain.
The methodology of the study was strong. The authors performed a prospective blinded cohort study to minimize bias. Strengths of the methodology include independent physical examinations by a board certified orthopedic surgeon and an orthopedics board certified physical therapist, detailed descriptions of the physical examination techniques, and arthroscopic examinations of all of the participants' shoulders (by another unaffiliated orthopedic surgeon) to validate the physical exam findings. Independently performed examinations minimized observer bias between testers and also provided the basis for determining the validity of the tests in clinical practice. The detailed descriptions of the physical examination techniques allow for future researchers to confirm or refute the results of the current study in other populations. Finally, post-operative reports from the arthroscopic analysis indicate the varied causes of subacromial impingement. Implications of these results on clinical practice are discussed in the sections below.
The study did have limitations. SIS is a general diagnosis - much like anterior knee pain of the lower extremity. There are numerous musculoskeletal (glenohumeral dykinesis) and structural causes (such as a hooked acromion) of SIS, independent of a neuromuscular coordination deficiency (such as underactive lower trapezius and an overactive upper trapezius causing excessive scapular elevation and anterior tipping). The current study did not exclude individuals with concomitant shoulder pathologies, which reduces the specificity of the cluster in clinical practice; however, the presence of other pathologies in conjunction with SIS is common. Second, the number of participants required to show statistical significance was determined to be 57 based on an a priori power analysis. The current study only had 55 participants complete the study, which increases the risk of a type I error (incorrect rejection of a true null hypothesis (a "false positive")), potentially overestimating the screening efficacy of the cluster for detection of SIS. Future studies on this topic should include enough participants to reduce the chance of a type I error.
Why is this study important?
SIS is commonly managed conservatively with strengthening and neuromuscular re-education; however, there are also numerous soft tissue, joint, and neural causes of shoulder pain that may present in conjunction with SIS that require referral for additional medical management. The current study provides an assessment cluster that can be used to rule in/rule out SIS with superior validity to any single SIS test. This may lead to more accurate assessment, and in-turn lead to more efficient and effective management and treatment of shoulder pain.
How does it affect practice?
The current study supports using the painful arc test , the empty can test , and the ERRT to rule in SIS when examining an individual with shoulder pain. If these three tests are positive, the clinician can confirm the diagnosis of SIS and proceed to further diagnostic testing to rule-out/rule-in other shoulder pathologies such as glenohumeral joint instability or rotator cuff tears. The results of the current study also suggest that if less than three of those tests are positive, SIS may be ruled-out. A negative Neer's test can further strengthen the clinician's ability to rule out SIS.
Combining the subjective assessment and physical examination findings (including this testing cluster) is likely the most sensitive and specific approach to diagnosing SIS, regardless of the validity of the testing cluster alone. Optimally, clinicians would integrate findings from both subjective exams and researched testing clusters.
The current study indicates that SIS usually presents with other concomitant shoulder pathologies such as labral tears, partial and full rotator cuff tears, and instability which may compromise the subacromial space. In practice, if these conditions have been ruled out, clinicians can be confident that conservative management through strengthening and neuromuscular re-education are indicated, and will likely reduce impingement symptoms, reduce pain, and improve function.
How does it relate to Brookbush Institute Content?
It is hypothesized that subacromial impingement syndrome (SIS) is the result of arthrokinematic dyskinesis of the glenohumeral joint , resulting in irritation/inflammation of subacromial tissues and pain. Further, this arthrokinematic dyskinesis is likely the result of one or more of a predictable set of compensations described in the Brookbush Institute predictive model of Upper Body Dysfunction (UBD) . As this impairment involves multiple joints, muscles, nerves and fascial structures, a thorough movement assessment is recommended before recommending an intervention/corrective program. Testing clusters like the one discussed in this study, are used by the Brookbush Institute to "clear" the patient/client for further assessment and treatment/exercise with a licensed practitioner. Although the results of the testing cluster may not imply specific interventions, they decrease the likelihood that a patient/client's time, financial resources, motivation and health are not squandered. In the case of the Michener et al. SIS Testing Cluster, positive results on 3 or more tests with negative results on all other shoulder pathologies tests, combined with an unremarkable subjective assessment, would imply that a patient/client is likely to improve under our care (Physical Therapists, Athletic Trainer, Chiropractor)
The following videos describe, demonstrate and discuss the tests used in this study: