
Research Review: Effect of Individual Strengthening Exercises for Posterior Pelvic Tilt Muscles on Back Pain, Pelvic Angle, and Lumbar ROM of a LBP Patient with Excessive Lordosis: A Case Study
By Corbin Henault MEd, ATC
Edited by Brent Brookbush, DPT, PT, COMT, MS, PES, CES, CSCS, H/FS
Original Citation: Yoo, W. G. (2014). Effect of the individual strengthening exercises for posterior pelvic tilt muscles on back pain, pelvic angle, and lumbar ROM of a LBP patient with excessive lordosis: a case study. Journal of physical therapy science, 26(2), 319-320. Article
Why the Study Is Relevant: Sacral inclination angle is often greater for low back pain (LBP) patients than when compared to a healthy population (1). There is no consensus on whether changing the pelvic inclination angle helps relieve LBP. This 2013 case study by a South Korean researcher, investigated the effects of strengthening exercises for the muscles responsible for posteriorly tilting the pelvis on anterior pelvic tilt (APT) angle, lumbar range of motion (ROM), and LBP in an individual with excessive lumbar lordosis. The results suggest that strengthening the rectus abdominis , gluteus maximus and hamstrings has a positive effect on LBP and APT angle.
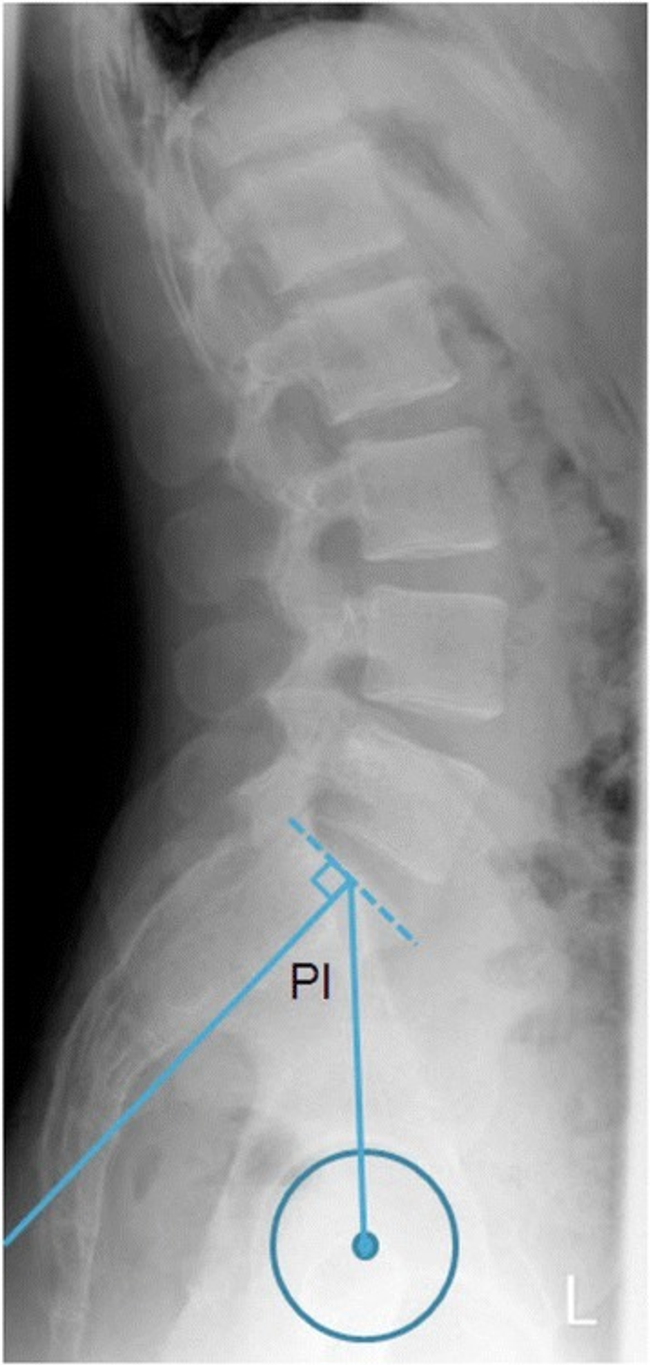
Lateral view of the lower spine and pelvis showing the pelvic incidence angle. Image: Tiziani S.-
https://openi.nlm.nih.gov/detailedresult.php?img=PMC4589032_12880_2015_80_Fig1_HTML&query=pelvic+angle&it=xg&req=4&npos=81
Study Summary
| Study Design | Case Study |
| Level of Evidence |
|
| Participant Characteristics | Demographics
Inclusion Criteria:
Exclusion Criteria:
|
| Methodology |
|
| Data Collection and Analysis |
|
| Outcome Measures |
|
| Results |
|
| Our Conclusions | The conclusion of the researchers reinforces the Brookbush Institute's recommendation that strengthening exercises for the muscles involved in posteriorly tilting the pelvic may aid in reducing anAPT and LB while increasing lumbar ROM. |
| Researchers' Conclusions | Strengthening muscles that encourage posterior pelvic tilt reduces LBP and APT while increasing lumbar ROM in individuals with LBP and excessive lordosis. |

Ultimate Glute Bridge
Review & Commentary: This study adds to the body of research concerning low back pain (LBP) and anterior pelvic tilt (APT), specifically the use of strengthening exercises to correct APT. The researcher applied a simple approach, selecting an intervention targeting a few key muscles responsible for posterior pelvic tilt with a single exercise for each muscle group.
The study had many methodological strengths, including:
- Validated instruments were used increasing confidence in study results. This includes the palpation meter and dual inclinometer, both with a reliability of .8 or higher (2, 3).
- The researcher was extremely thorough in describing the methodology, measurements and exercise protocols. Any movement professional should be able to replicate the study.
- The simple approach is easily applied to practice, and lends itself to easy replication in larger studies.
- The participants did not receive any previous treatment for low back pain which could have confounded outcomes.
Weaknesses that should be noted prior to clinical integration include:
- The two-week intervention period may be insufficient to imply long-term effects of the exercise protocol.
- While the study results are encouraging, the next step should be replicating this study in a larger population of participants who report LBP with APT and excessive lordosis.
- The visual analogue score (VAS) may not be the most valid instrument for reporting pain (4), the addition of a validated outcome measure questionnaire may be beneficial in future studies.
How This Study is Important:
This study adds to a growing body of research on treatment strategies for LBP. Specifically, this case study examined the effectiveness of exercises that target muscles that will posteriorly tilt the pelvis. The specificity of exercise selection differs from those studies that examine exercise with the more general intent of “core stabilization." These findings demonstrate that a major change in pelvic tilt, lumbar spine angle and LBP can be achieved in a short period of time through targeted strengthening exercises. This information provides human movement professionals with an evidence base to support choosing core exercise that targets muscles that will posteriorly tilt the pelvis.
How the Findings Apply to Practice:
Non-specific chronic LBP is a prevalent and complicated issue that should be addressed using an integrated treatment model (holistic approach) (5). Exercise selection should address both stability and mobility issues, as well as specific movement impairments, as illustrated by this case study. Human Movement Professionals should consider addressing lumbar flexor and hip extensor strength in those with LBP, excessive lordosis and anterior pelvic tilt.
How does it relate to Brookbush Institute Content?
The findings of this study indicate that LBP, anterior pelvic tilt and excessive lordosis can be corrected with individual strengthening exercises for the rectus abdominis , gluteus maximus and hamstrings . This is in large part consistent with recommendations within the Brookbush Institute's predictive models for Lumbo Pelvic Hip Complex Dysfunction (LPHCD) , Lumbosacral Dysfunction (LSD) and Lower Extremity Dysfunction (LED) . The gluteus maximus is described as long and under-active in individuals with LPHCD; however, the rectus abdominis and biceps femoris are described as long and over-active and recommended that release and integrated strengthening, rather than specific strengthening, should be used to address these muscles. Further, transverse abdominis activation would be recommended to reduce synergistic dominance of the lumbar flexors. The Brookbush Institute would humbly welcome a comparative study of the two approaches. As such, human movement professionals are encouraged to release the biceps femoris , apply individual strengthening exercises for the gluteus maximus , and test the effectiveness of lumbar flexor versus transverse abdominis activation when rehabilitating or correcting LBP, anterior pelvic tilt and excessive lordosis in clients.
The following videos demonstrate the overhead squat assessment for anterior pelvic tilt, gluteus maximus isolated activation, and self-administered (SA) static release technique for the biceps femoris:
Overhead Squat Assessment - Anterior Pelvic Tilt (Excessive Lordosis):
Transverse Abdominis
Gluteus Maximus Isolated Activation:
Biceps Femoris SA Static Release:
Bibliography:
- Evcik, D., & Yücel, A. (2003). Lumbar lordosis in acute and chronic low back pain patients. Rheumatology international, 23(4), 163-165.
- Petrone, M. R., Guinn, J., Reddin, A., Sutlive, T. G., Flynn, T. W., & Garber, M. P. (2003). The accuracy of the palpation meter (PALM) for measuring pelvic crest height difference and leg length discrepancy. Journal of orthopaedic & sports physical Therapy, 33(6), 319-325.
- Sangtarash, F., Manshadi, F. D., Sadeghi, A., Tabatabaee, S. M., & Gheysari, A. M. (2014). Validity and reliability of dual digital inclinometer in measuring thoracic kyphosis in women over 45 years . J Spine, 3(170), 2.
- Carlsson, A. M. (1983). Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale . Pain, 16(1), 87-101.
- O’Sullivan, P. (2012). It’s time for change with the management of non-specific chronic low back pain . Br J Sports Med, 46(4), 224.
© 2017 Brent Brookbush
Questions, comments, and criticisms are welcomed and encouraged -