
Research Review: Posterior Glenohumeral Mobilizations Increase Internal Rotation Range of Motion
By Nicholas Rolnick SPT, MS, CSCS
Edited by Brent Brookbush DPT, PT, COMT, MS, PES, CES, CSCS, ACSM H/FS
Original Citation: Yu IY, Jung IG, Kand MH et al. Immediate effects of an end-range mobilization technique on shoulder range of motion and skin temperature in individuals with posterior shoulder tightness. J Phys Ther Sci. 2015; 27: 1723-1725. ARTICLE
Why the Study is Relevant: Human movement professionals in rehab, fitness and performance settings use glenohumeral joint mobilizations to improve shoulder range of motion and/or reduce pain. In rounded shoulders with forward head posture, the posterior capsule of the glenohumeral joint is frequently stiff, resulting in a loss of internal rotation (1). Loss of shoulder range of motion predisposes individuals to shoulder injuries, including rotator cuff tears and shoulder impingement (2). In this 2015 study, Korean researchers used digital infrared thermographic imaging to investigate the immediate effects of a grade IV posterior glenohumeral joint mobilization on range of motion and blood flow in 13 individuals with internal rotation deficits. The results indicate that posterior glenohumeral mobilizations significantly improves internal rotation range of motion as well as localized blood flow to the shoulder . These results suggest that the benefits of joint mobilization may be attributed to neurophysiological factors.
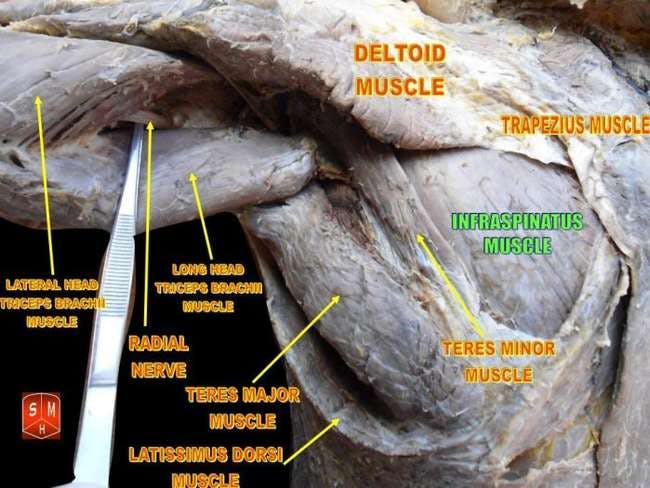
The posterior capsule is commonly defined as being composed of infraspinatus, teres minor, and the posterior deltoid. Stiffness in the posterior capsule has been theorized to produce restrictions in internal rotation range of motion. -By Anatomist90 - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=17900187
Study Summary
| Study Design | Cohort Study |
| Level of Evidence | IIA Evidence from at least one controlled study without randomization |
| Methodology |
|
| Outcome Measures |
|
| Results |
|
| Our Conclusions | Posterior glenohumeral joint mobilizations are effective at improving shoulder joint extensibility in individuals with upper body dysfunction. |
| Researchers' Conclusions | Grade IV posterior glenohumeral joint mobilizations are effective at increasing glenohumeral internal rotation range of motion and skin temperature in individuals with posterior shoulder girdle tightness. |

For human movement professionals whose scope of practice does not include manual joint mobilizations, the Brookbush Institute recommends this technique for similar benefits.
Review & Commentary:
The study was the first of its kind to compare the effects of a grade IV posterior glenohumeral joint mobilization on internal rotation range of motion and skin temperature. The use of skin temperature measurements allowed the authors to investigate a potential mechanism (increased blood flow, temperature linked changes to soft-tissue extensibility) responsible for the increased posterior capsule extensibility. This study adds to the body of literature suggesting that joint mobilizations can significantly improve range of motion.
Methodological strengths were many, including:
- Appropriate inclusion/exclusion criteria were important for excluding individuals who would not normally benefit from the intervention. Posterior glenohumeral joint mobilizations are commonly indicated for individuals with restrictions in internal rotation and/or flexion range of motion (1). Narrowing the participants to only those individuals with restrictions allowed researchers to determine the immediate effect of this technique on clinically appropriate outcomes.
- Posterior glenohumeral joint mobilizations have been taught for decades and are often used in a clinical setting. The investigation of such a commonly used technique infers the clinical relevance of this study.
- Because the mechanisms behind joint mobilizations are still unknown, combining skin temperature measurements on five different points on the shoulder provided an indirect way to measure the autonomic nervous system's response to a manual therapy intervention. The results of the current study indicate that skin temperature changes do occur in the region of the joint mobilization and could be a factor in reducing of muscle spasms and soft tissue tightness. More research is needed.
Weaknesses that should be noted prior to clinical integration of the findings include:
- Although this study was the first of its kind to test the immediate effects of a posterior glenohumeral joint mobilization on shoulder internal rotation range of motion in clinically appropriate individuals, much is unknown about the study's methodology. The authors did not conduct a reliability study prior to the start of the study, or comment on the use of methods that have been found to be reliable in previous studies (for example, the reliability of goniometry ). Without knowing the reliability of the measurements taken for either the internal rotation range of motion or the skin temperature measurements, the results of the current study must be taken with caution. Future studies should perform reliability assessments to strengthen results.
- There were no descriptions given of the grade IV posterior glenohumeral joint mobilization and placement of the skin temperature recorders protocols. Traditionally, grade IV mobilizations are a small amplitude, rhythmic oscillating force at the end-range of movement (5). However, there are sources that describe the intervention differently, which may alter clinical outcomes Similarly, without precise locations of the skin temperature recorders, replication of the study will be difficult. Future research should clearly describe all important aspects of the methodology.
- Short-term nature of the intervention. Few conclusions can be drawn about long-term effects. Future studies should include a follow-up period that is typical of clinical practice (i.e., 2-4 days, 2-4 weeks, 6 -12 months).
Why This Study Is Important
The results of the study support the efficacy of manual glenohumeral joint mobilization in individuals with internal rotation range of motion deficits. Increased skin temperature in the posterolateral shoulder, post-intervention, suggests that joint mobilizations may stimulate a reflexive sympathetic response from the autonomic nervous system (4). Increased blood flow to the area could suggest that tissue response to mobilization is primarily neurophysiological response rather than mechanical. More research on the topic is needed. The study lays the groundwork for further investigation into the effects of glenohumeral joint mobilizations on clinical outcomes.
How the Findings Apply to Practice
The findings suggest that in individuals with posterior shoulder tightness, posterior glenohumeral joint mobilizations at end-range internal rotation are effective at increasing internal rotation range of motion. Internal rotation improved approximately 13° on average (from 42.08° to 55.7°), which is both statistically and clinically significant. Human movement professionals assessing individuals with internal rotation range of motion deficits () should consider using this technique if it is within the scope of practice and muscular causes have been ruled out.
Related Brookbush Institute Content
Manual therapists are taught that posterior glenohumeral joint mobilizations can improve shoulder internal rotation and shoulder flexion range of motion. The Brookbush Institute recommends shoulder joint mobilizations to improve internal rotation range of motion deficits when posterior deltoid , infraspinatus and teres minor muscular restrictions have been ruled out, or have been treated but outcomes are less than optimal. These muscles are commonly affected in individuals with upper body dysfunction and should be released and stretched to restore optimal joint extensibility. The study did not employ any release or lengthening techniques for the posterior deltoid prior to the intervention, which may have improved internal rotation range of motion further. It may be interesting to compare release and mobilization, to mobilization and release techniques alone in a future study. The Brookbush Institute's model of addressing postural dysfunction is comprehensive (integrative), involving a sequential progression of release, mobilization and lengthening techniques to enhance mobility, and activation and integration techniques to increase activity and strength of under-active muscles with intent of optimizing motion and posture.
To determine effectiveness of the mobilization, the Brookbush Institute recommends the procedure of "assess, intervention and re-assess." In the case of shoulder internal rotation range of motion restrictions, recording shoulder internal rotation and/or shoulder flexion using a goniometer prior to joint mobilization can provide objective data on the efficacy of the intervention.
Human movement professionals (DPT, DCs, ATCs) whose scope of practice includes manual therapy can utilize posterior glenohumeral joint mobilizations to improve joint range of motion. Forthcoming videos will focus on manual mobilization techniques including posterior glenohumeral joint mobilizations. Human movement professionals can accomplish similar goals with clients through self-administered general shoulder joint mobilizations .
The following videos illustrate common assessment techniques and interventions used to treat shoulder internal rotation range of motion restrictions.
Brookbush Institute Videos
Shoulder Flexion Goniometry
Shoulder Internal Rotation Goniometry
Self-Administered Posterior Shoulder Release
Self-Administered Shoulder Mobilization
Posterior Shoulder Stretch (Sleeper Stretch)
References:
- Duzgun I, Turgut E, Cinar-Medeni, et al. The presence and influence of posterior capsule tightness on different shoulder problems. J Back Musculoskelet Rehabil. June 2016;
- Kolber MJ, Hanney WJ, Cheatham SW, et al. Shoulder joint and muscle characteristics among weight-training participants with and without impingement syndrome. J Strength Cond Res. July 2016;
- Park JY, Hyun JK, Seo JB. The effectiveness of digital infrared thermographic imaging in patients with shoulder impingement syndrome. J Shoulder Elbow Surg. 2007; 16: 548-554.
- Petersen N, Vicenzino B, Wright A. The effects of a cervical mobilization technique on sympathetic outflow to the upper limb in normal subjects. Physiother Theory Pract. 1993; 9: 149–56.
- Mintken PE, et al. A Model for Standardizing Manipulation Terminology in Physical Therapy Practice. J Orthop Sports Phys Ther. 2008; 38(3):A1-A6.
© 2016 Brent Brookbush
Questions, comments, and criticisms are welcomed and encouraged -